 Spiders never were any good at statistics.
Spiders never were any good at statistics. Related to the post below, a second study was floating around the interweb last week, which is worth looking at. It caused a stir in a number of health and fitness circles as a “hallelujah” moment, and came tagged with headlines such as:
Is it true? Can we finally put down the statins and pick up our running shoes in the knowledge that it will make us live just as long? Well, you should, obviously, but not on the back of this study. As much as it pains me, I can safely say that this study tells us nothing useful about how well drugs compare to exercise in the treatment of disease. However, this is not the fault of the researchers, as I’ll try to explain.
In this study, two people who work at the London School of Economics, Harvard and Stanford analysed all the studies that have ever compared drugs to placebo or exercise. Their focus was studies which looked at a reduction in mortality (risk of death). They included only randomised-controlled trials (RCTs) and meta-analyses, which are the “gold standard” of evidence-based medicine. An RCT takes a patient and randomises them to one treatment or another. This aims to remove any bias that a doctor may have in terms of which patients get which treatment, and means the groups you compare are as equal as possible. A meta-analysis takes all the trials of a specific treatment, and groups them together. If a treatment has a very small effect, it may not show up in one trial, but if you put all the trials together you might then end up with enough patient numbers to see the effect.
The introduction to this study tells us that exercise has been shown to reduce the effects of arthritis, heart disease, diabetes and cancer, as I discussed briefly yesterday. Then there follows some sobering statistics:
Clearly we are 50% sicker now than we were ten years ago.
When searching for trials and meta-analyses, they found data on four diseases where exercise was used as a potential way to reduce the risk of death:
This is where things become very abstract. Very few trials or meta-analyses compared exercise directly with drug therapy. In fact, only one study of the 16 meta-analyses and 305 RCTs they found compared exercise to a drug. Drugs were usually compared to other drugs or to placebo, and exercise was usually compared to “control”. This means that exercise was either:
a) compared to not getting any increase in exercise, or
b) added in to “best practice” medical (drug) therapy for that disease. Standard therapy plus exercise was then compared to standard therapy alone.
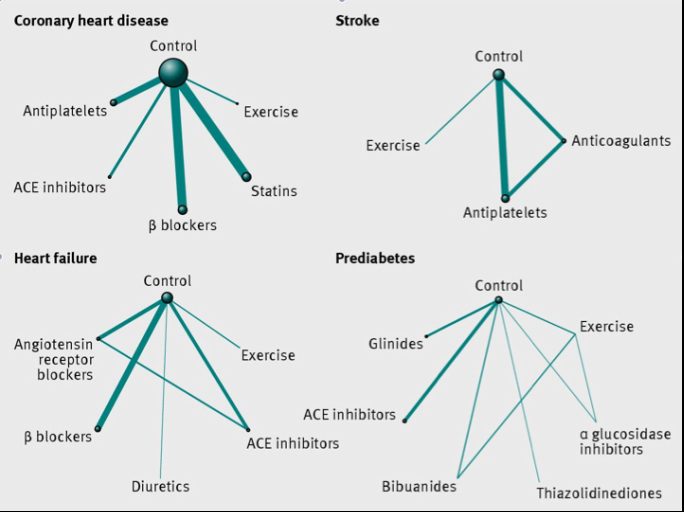
Because of this, they had no choice but to put all the treatments together into a large statistical analysis, and merely infer whether exercise might be better or worse than a drug at reducing mortality, even though they have never been compared directly. They even produced some complicated spider diagrams to show how hard they tried (see below). The lines show what was compared to what, and the thickness of the line implies the strength of the evidence. The “exercise” line is always pretty anaemic, regardless of the disease.
So, what did they find?
Stroke: Compared to common drug treatments after stroke, exercise was significantly better at reducing the risk of death. Not just a bit better, either. Those who were in the exercise trials were 90% less likely to die than those on drug treatments.
HOLD. THE. PHONE. That’s incredible!
Not so fast – These numbers come from a total of three trials examining the effect of exercise in 227 patients. This is compared to 27 drug trials totalling 77,394 patients. The thing about a stroke is that it will rarely kill you. Rather, it’s usually either the heart attack that you’re also at risk of, or the fact that you can’t control your body fully any more. This means you fall over and fracture your hip. Or choke on (“aspirate”) your food and get a bad pneumonia. The patients in drug trials tended to be enrolled within two days of a stroke, whereas the exercise patients started treatment up to 150 days after their stroke. Those that are fit enough to begin exercise after five months are already going to perform better. This is obviously a preferable outcome for the patient, but comparing them to the sicker patients in drug trials isn’t really fair.
Heart Failure: In heart failure, the study found no beneficial effect of exercise compared to any of the drugs they examined. Heart failure is one area where drugs do show an unparalleled survival benefit, and the same was seen here.
Heart Disease and Pre-Diabetes: In those with heart disease, all the drugs examined reduced the risk of mortality by 15-20%. A similar reduction in mortality was seen with exercise, but the effect was not statistically significant. As was the case with stroke, 5,685 patients across the analysis were randomised to exercise. This is compared to 81,655 who received a drug intervention. The numbers are so unbalanced that it’s no wonder they couldn’t find a significant effect! When they then compared all the drugs with exercise in their fancy “network meta-analysis”, none of the treatments (including exercise) were significantly better than any other. The same was seen in pre-diabetes.
Now you COULD rush out and tell the world that “exercise is as good as medication”, but that’s not what the study shows. It only really tells us that so few patients have been put in trials involving exercise (and almost none that actually compare drugs to exercise) that it is impossible to find an effect. This point is actually re-iterated by the authors in their conclusion:
“Perhaps unsurprisingly, the amount of evidence on the mortality benefits of exercise is considerably smaller than that on drug interventions…. and highlight the changing landscape of research, which seems to increasingly favour drug interventions over strategies to modify lifestyle. The current body of medical literature largely constricts clinicians to drug options.”
Let’s consider why this might be the case. Your average general practitioner is told that exercise improves all the diseases listed above. But what should they tell you to do?
Exercise guidance does not form part of the medical education given to doctors and they therefore cannot be expected to be authorities on the subject. From experience, it appears that most doctors don’t know anything about what kind of exercise improves health. If that’s the case, how can they be expected to provide accurate, easy-to-follow guidelines for their patients? Only once this information pervades the clinical psyche will we maybe be able to get together enough patients to show an effect in trials.
However, there is more and more pressure in this area, and there will hopefully come a day where drug companies will be forced to compare their products to structured changes in diet and exercise in order to see which is truly better at improving disease outcomes.
On that positive note, my next post will cover the training types which have been proven to improve health.
References
1. Naci H and Ioannidis JPA. Comparative effectiveness of exercise and drug interventions on mortality outcomes: metaepidemiological study. BMJ 2013;347:f5577
- “Exercise 'can be as good as pills'”
- “Exercise As Effective As Drugs For Treating Heart Disease, Diabetes”
Is it true? Can we finally put down the statins and pick up our running shoes in the knowledge that it will make us live just as long? Well, you should, obviously, but not on the back of this study. As much as it pains me, I can safely say that this study tells us nothing useful about how well drugs compare to exercise in the treatment of disease. However, this is not the fault of the researchers, as I’ll try to explain.
In this study, two people who work at the London School of Economics, Harvard and Stanford analysed all the studies that have ever compared drugs to placebo or exercise. Their focus was studies which looked at a reduction in mortality (risk of death). They included only randomised-controlled trials (RCTs) and meta-analyses, which are the “gold standard” of evidence-based medicine. An RCT takes a patient and randomises them to one treatment or another. This aims to remove any bias that a doctor may have in terms of which patients get which treatment, and means the groups you compare are as equal as possible. A meta-analysis takes all the trials of a specific treatment, and groups them together. If a treatment has a very small effect, it may not show up in one trial, but if you put all the trials together you might then end up with enough patient numbers to see the effect.
The introduction to this study tells us that exercise has been shown to reduce the effects of arthritis, heart disease, diabetes and cancer, as I discussed briefly yesterday. Then there follows some sobering statistics:
- Only 14% of adults in the UK exercise regularly.
- Only 33% meet minimum recommended levels of activity.
- On average, every person gets nearly 18 drug prescriptions per year.
- The number of prescriptions has increased by 50% from 2000 to 2010.
Clearly we are 50% sicker now than we were ten years ago.
When searching for trials and meta-analyses, they found data on four diseases where exercise was used as a potential way to reduce the risk of death:
- Secondary prevention of heart disease (ie those with previous heart attacks).
- Heart failure.
- Strokes.
- Pre-diabetes (those with impaired glucose control, but before full-blown diabetes).
This is where things become very abstract. Very few trials or meta-analyses compared exercise directly with drug therapy. In fact, only one study of the 16 meta-analyses and 305 RCTs they found compared exercise to a drug. Drugs were usually compared to other drugs or to placebo, and exercise was usually compared to “control”. This means that exercise was either:
a) compared to not getting any increase in exercise, or
b) added in to “best practice” medical (drug) therapy for that disease. Standard therapy plus exercise was then compared to standard therapy alone.
Because of this, they had no choice but to put all the treatments together into a large statistical analysis, and merely infer whether exercise might be better or worse than a drug at reducing mortality, even though they have never been compared directly. They even produced some complicated spider diagrams to show how hard they tried (see below). The lines show what was compared to what, and the thickness of the line implies the strength of the evidence. The “exercise” line is always pretty anaemic, regardless of the disease.
So, what did they find?
Stroke: Compared to common drug treatments after stroke, exercise was significantly better at reducing the risk of death. Not just a bit better, either. Those who were in the exercise trials were 90% less likely to die than those on drug treatments.
HOLD. THE. PHONE. That’s incredible!
Not so fast – These numbers come from a total of three trials examining the effect of exercise in 227 patients. This is compared to 27 drug trials totalling 77,394 patients. The thing about a stroke is that it will rarely kill you. Rather, it’s usually either the heart attack that you’re also at risk of, or the fact that you can’t control your body fully any more. This means you fall over and fracture your hip. Or choke on (“aspirate”) your food and get a bad pneumonia. The patients in drug trials tended to be enrolled within two days of a stroke, whereas the exercise patients started treatment up to 150 days after their stroke. Those that are fit enough to begin exercise after five months are already going to perform better. This is obviously a preferable outcome for the patient, but comparing them to the sicker patients in drug trials isn’t really fair.
Heart Failure: In heart failure, the study found no beneficial effect of exercise compared to any of the drugs they examined. Heart failure is one area where drugs do show an unparalleled survival benefit, and the same was seen here.
Heart Disease and Pre-Diabetes: In those with heart disease, all the drugs examined reduced the risk of mortality by 15-20%. A similar reduction in mortality was seen with exercise, but the effect was not statistically significant. As was the case with stroke, 5,685 patients across the analysis were randomised to exercise. This is compared to 81,655 who received a drug intervention. The numbers are so unbalanced that it’s no wonder they couldn’t find a significant effect! When they then compared all the drugs with exercise in their fancy “network meta-analysis”, none of the treatments (including exercise) were significantly better than any other. The same was seen in pre-diabetes.
Now you COULD rush out and tell the world that “exercise is as good as medication”, but that’s not what the study shows. It only really tells us that so few patients have been put in trials involving exercise (and almost none that actually compare drugs to exercise) that it is impossible to find an effect. This point is actually re-iterated by the authors in their conclusion:
“Perhaps unsurprisingly, the amount of evidence on the mortality benefits of exercise is considerably smaller than that on drug interventions…. and highlight the changing landscape of research, which seems to increasingly favour drug interventions over strategies to modify lifestyle. The current body of medical literature largely constricts clinicians to drug options.”
Let’s consider why this might be the case. Your average general practitioner is told that exercise improves all the diseases listed above. But what should they tell you to do?
Exercise guidance does not form part of the medical education given to doctors and they therefore cannot be expected to be authorities on the subject. From experience, it appears that most doctors don’t know anything about what kind of exercise improves health. If that’s the case, how can they be expected to provide accurate, easy-to-follow guidelines for their patients? Only once this information pervades the clinical psyche will we maybe be able to get together enough patients to show an effect in trials.
However, there is more and more pressure in this area, and there will hopefully come a day where drug companies will be forced to compare their products to structured changes in diet and exercise in order to see which is truly better at improving disease outcomes.
On that positive note, my next post will cover the training types which have been proven to improve health.
References
1. Naci H and Ioannidis JPA. Comparative effectiveness of exercise and drug interventions on mortality outcomes: metaepidemiological study. BMJ 2013;347:f5577
 RSS Feed
RSS Feed