Calorie counting doesn’t work. So fuck*ng stop it. Now.
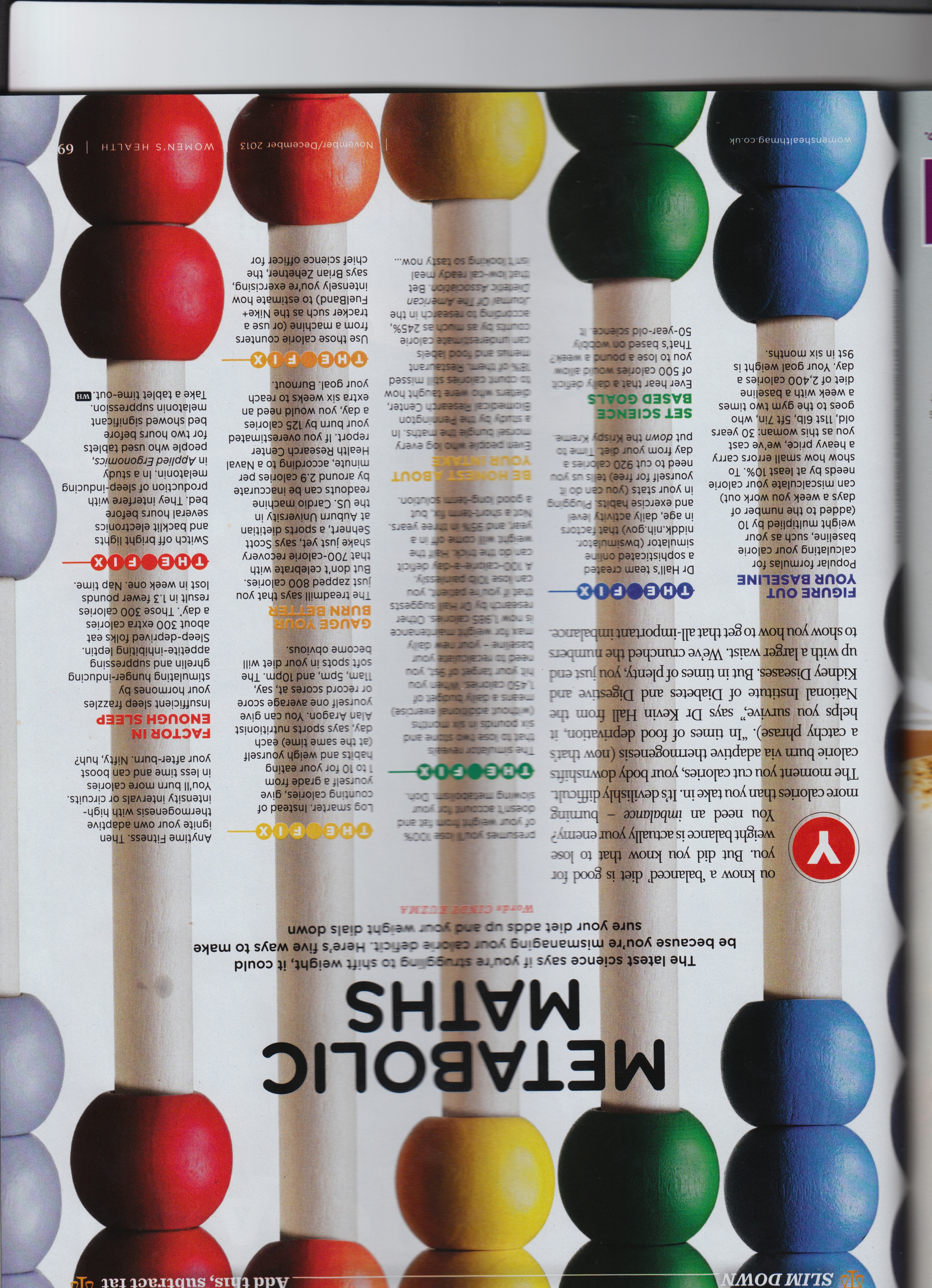
For many people, this may not be new. The internet is full of stories about how “a calorie is not a calorie”, and how inaccurate “counting calories” can be when trying to lose weight. However, we STILL get nonsense like this article in a magazine that claims to be for the benefit of women’s health:
For many people, this may not be new. The internet is full of stories about how “a calorie is not a calorie”, and how inaccurate “counting calories” can be when trying to lose weight. However, we STILL get nonsense like this article in a magazine that claims to be for the benefit of women’s health:
| metabolic_maths.jpeg |
It starts by telling you how your calorie counting probably isn’t getting you the fat loss you want, and how to count calories “better”. Elsewhere they even give us the great news of some cakes “under 200 calories”, and how many minutes we should spend on the treadmill to “burn off” various meals.
There are over 300 “calorie counting” apps available for the iPhone, but almost nobody talks about what a Calorie actually is. Broadly speaking, a Calorie is the heat needed to raise the temperature of 1 kg of water by 1°C.
You may notice that “Calorie” in the definition a capital “c”. The Calories (capital c) that we use in nutrition are actually kilocalories, the equivalent of 1,000 calories (little c), but the capital letter is usually dropped, for simplicity. The Calorie is a measure of energy, which makes sense. However, once you know how the calories in food are measured, it becomes clear that it’s not as simple as the magazines would like you to think.
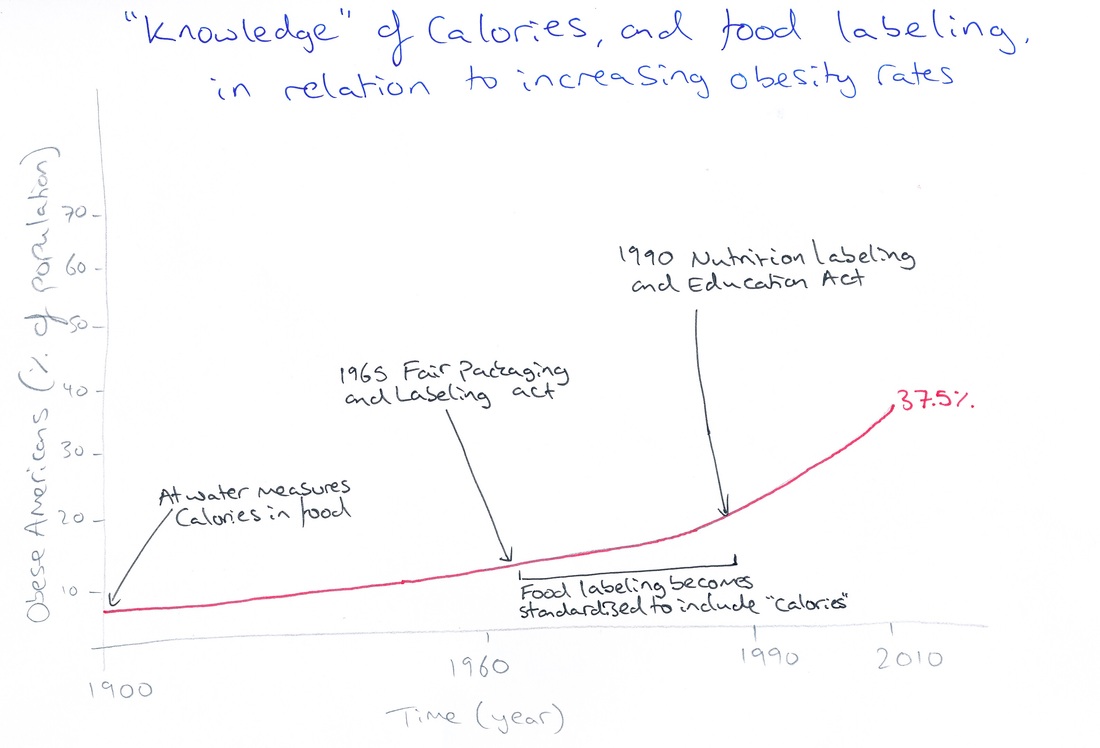
Wilbur Atwater established the system for determining the calorie content of foods in 1900. In an instrument called a calorimeter, Atwater basically set fire to food, placed a beaker of water on top, and measured how much the temperature of the water increased by. Using the definition above, Atwater could then calculate how many “Calories” were in certain foods. Just looking at that, some flaws seem evident. The whole premise assumes that we take in 100% of the energy in our food by “burning” it until we get ash. I don’t have to tell you that the human body is a little more sophisticated than that…
Based on Atwater’s studies, it became widely accepted that carbohydrates and proteins have 4 Calories per gram, and fat has 9 Calories per gram. However, since the 1950s we have known that the values for different types of protein can vary by 10-20%, and carbohydrates can vary up to 50%. Even so, manufacturers nowadays simply calculate the amount of fat, protein or carbohydrate in their food, multiply by the Atwater factors, and put that number of “calories” on the packet.
Earlier this year, a conference held by American Association for the Advancement of Science discussed “Why a Calorie Is Not a Calorie and Why It Matters for Human Diets”. Speakers talked about how cooking, digestion, and hormones will all affect the number of “calories” we get from our food. The energy you get from a given meal could be up to 50% different from what the packet says!
This could go some way towards explaining why calorie-controlled diets just don’t provide sustained weight loss. A meta-analysis by Marion Franz and colleagues showed that long-term studies based around simple weight loss advice, including cutting calorie intake, result in no weight loss at all. Dramatically slashing the number of calories in the diet results in rapid weight loss over the first six months, but most of this is regained again within two years. And these are people regularly getting input from dieticians and doctors.
Imagine how the poor sods trying to survive on low-calorie cereal bars and sheer willpower are going to fare.
In fact, my beautifully unscientific graph shows that knowing and thinking about calories, as has become synonymous with any attempt at staying “healthy” and losing weight, has had no effect on rates of obesity:
There are over 300 “calorie counting” apps available for the iPhone, but almost nobody talks about what a Calorie actually is. Broadly speaking, a Calorie is the heat needed to raise the temperature of 1 kg of water by 1°C.
You may notice that “Calorie” in the definition a capital “c”. The Calories (capital c) that we use in nutrition are actually kilocalories, the equivalent of 1,000 calories (little c), but the capital letter is usually dropped, for simplicity. The Calorie is a measure of energy, which makes sense. However, once you know how the calories in food are measured, it becomes clear that it’s not as simple as the magazines would like you to think.
Wilbur Atwater established the system for determining the calorie content of foods in 1900. In an instrument called a calorimeter, Atwater basically set fire to food, placed a beaker of water on top, and measured how much the temperature of the water increased by. Using the definition above, Atwater could then calculate how many “Calories” were in certain foods. Just looking at that, some flaws seem evident. The whole premise assumes that we take in 100% of the energy in our food by “burning” it until we get ash. I don’t have to tell you that the human body is a little more sophisticated than that…
Based on Atwater’s studies, it became widely accepted that carbohydrates and proteins have 4 Calories per gram, and fat has 9 Calories per gram. However, since the 1950s we have known that the values for different types of protein can vary by 10-20%, and carbohydrates can vary up to 50%. Even so, manufacturers nowadays simply calculate the amount of fat, protein or carbohydrate in their food, multiply by the Atwater factors, and put that number of “calories” on the packet.
Earlier this year, a conference held by American Association for the Advancement of Science discussed “Why a Calorie Is Not a Calorie and Why It Matters for Human Diets”. Speakers talked about how cooking, digestion, and hormones will all affect the number of “calories” we get from our food. The energy you get from a given meal could be up to 50% different from what the packet says!
This could go some way towards explaining why calorie-controlled diets just don’t provide sustained weight loss. A meta-analysis by Marion Franz and colleagues showed that long-term studies based around simple weight loss advice, including cutting calorie intake, result in no weight loss at all. Dramatically slashing the number of calories in the diet results in rapid weight loss over the first six months, but most of this is regained again within two years. And these are people regularly getting input from dieticians and doctors.
Imagine how the poor sods trying to survive on low-calorie cereal bars and sheer willpower are going to fare.
In fact, my beautifully unscientific graph shows that knowing and thinking about calories, as has become synonymous with any attempt at staying “healthy” and losing weight, has had no effect on rates of obesity:
I’m not suggesting that we get rid of “calories” completely. People should engage with what is in their food and where it comes from. Focusing on calories does also have its place. For example, increasing intake of calorie-dense foods in those who are dangerously underweight can be beneficial. In addition, radical calorie restriction in those that need rapid weight loss (ie before surgery in the morbidly obese) can be used if it is considered critical for the patient’s health.
For most people, though, health through sustainable weight loss will only come from sensible exercise, and a diet based around eating real food.
For most people, though, health through sustainable weight loss will only come from sensible exercise, and a diet based around eating real food.

This is not real food.
A more sensible approach
Purely counting “calories” cannot produce long-term weight loss because what your food is made of has a huge impact on your hormones and metabolism. The “energy is energy” argument doesn’t hold, because of the vast array of different reactions that will occur based on what you actually ate.
The most influential dietary factor that affects our ability to lose or gain weight is the amount of carbohydrate we consume. Some large studies in the USA have shown how carbohydrate intake maps closely with both obesity and type II diabetes:
Purely counting “calories” cannot produce long-term weight loss because what your food is made of has a huge impact on your hormones and metabolism. The “energy is energy” argument doesn’t hold, because of the vast array of different reactions that will occur based on what you actually ate.
The most influential dietary factor that affects our ability to lose or gain weight is the amount of carbohydrate we consume. Some large studies in the USA have shown how carbohydrate intake maps closely with both obesity and type II diabetes:
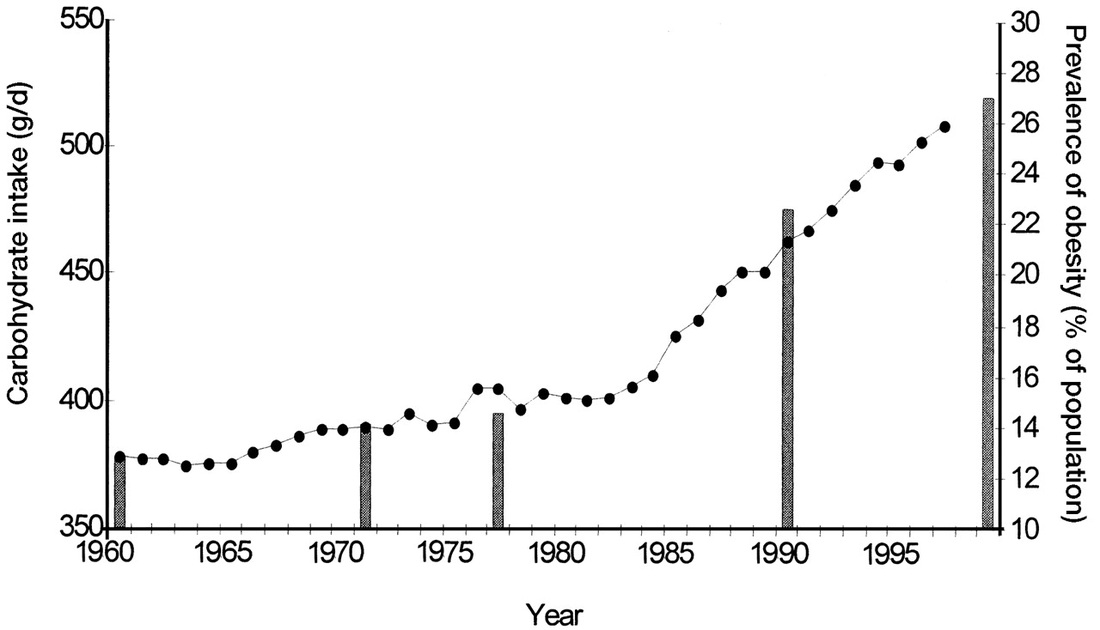
From Gross et al., 2004 (reference 6).
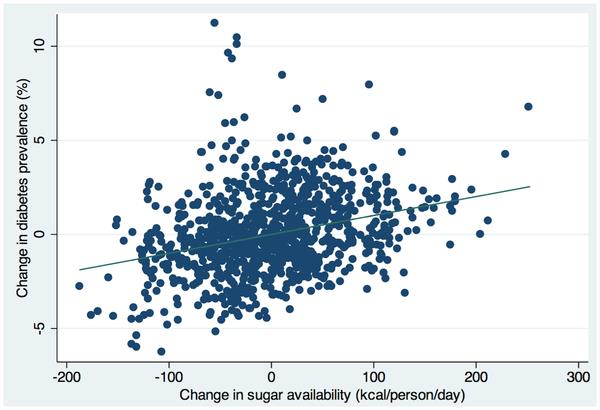
From Basu et al., 2004 (reference 7).
There is a huge “low-carb” diet debate that I will cover in the future, but a multitude of studies have examined low-carbohydrate, high-fat diets. These tend to be compared to low-fat, high-carbohydrate diets. In those that eat the same number of calories, participants on low carbohydrate diets:
With any weight loss, blood pressure, blood lipids and insulin/glucose control will almost always improve. In those who control their carbohydrate intake, this improvement is better than that seen in low-fat dieters who have lost the same amount of weight. Though those eating very few carbohydrates do often see an increase in “bad” LDL cholesterol, it changes to the larger, fluffier kind of LDL that is not associated with cardiovascular disease.
For those of you that still follow the “low-fat” mantra – there is an overwhelming change in blood lipids in those eating fewer carbohydrates and more fat, which is associated with reduced risk of heart attacks and strokes. This isn’t seen in low fat dieters, despite their weight loss.
In order for our fat cells to lay down more storage material as extra “cushioning”, they need insulin. Insulin is the hormone that our bodies produce primarily in response to carbohydrates. Insulin turns off the mechanism by which the body burns its fat stores for energy (lipolysis). Insulin also switches on the enzyme lipoprotein lipase, which sucks up all the fat from the meal you just ate, and uses it to make some extra padding for your jeans.
It follows, then, that by not eating as many carbohydrates with our meals, we don’t get the associated increase in insulin, and fat cells don’t get their “storage” switch turned on. In fact, if you give people a large fatty meal, those that have been following a low carbohydrate/high fat diet will have lower levels of fat in the blood afterwards, because the body has become used to using fat directly as a fuel source.
While we’re here, don’t think you can cheat the system by drinking “diet” soft drinks. Artificial sweeteners can also cause an increase in insulin, despite not containing any “calories” or carbohydrate.
Protein, metabolism and calorie restriction
You can’t trick the body into sudden weight loss. Our bodies will use energy and burn fat based on our metabolism. This is affected by the amount and types of food we eat, the exercise we do, and the amount of energy it takes to keep our organs and muscles running. If you rapidly reduce the amount of food you eat, the body will automatically reduce its metabolism in order to prevent huge changes in weight. This often involves sacrificing our muscle tissue. Muscles provide a large portion of our metabolism, and a healthy metabolism is essential to achieve fat loss.
Chronic dieters who restrict calories tend to lose weight, which will include some muscle tissue. They will then re-gain the weight due to a combination of a slower metabolism, and the fact that forcing yourself to eat less is miserable. Over time, their percentage bodyfat increases, as cycles of weight loss result in less muscle and a slower metabolism.
This effect can be reduced by increasing protein in the diet. The combination of increasing protein and reducing carbohydrate during weight loss leads to an increased proportion of weight lost from fat rather than muscle. Those following low-carbohydrate, high-fat diets also have a better preservation of muscle mass and smaller reduction in metabolic rate compared to high-carbohydrate, low-fat dieters.
Protein has the bonus of making you feel full for longer by increasing a hormone called peptide YY, which improves feelings of satiety. Protein also does not induce the same insulin spikes and troughs which give you that feeling of being starving an hour after eating your breakfast cereal.
- Lose at least as much weight, and up to twice as much weight compared to low fat dieters.
- Lose more weight from fat and retain more muscle, with a higher metabolic rate.
- Have lower levels of triglycerides and saturated fat in the blood, even though they eat more than three times as much saturated fat.
- Have higher HDL (“good”) cholesterol.
- Have better insulin and glucose tolerance, with reduced tendency to type II diabetes and metabolic syndrome.
With any weight loss, blood pressure, blood lipids and insulin/glucose control will almost always improve. In those who control their carbohydrate intake, this improvement is better than that seen in low-fat dieters who have lost the same amount of weight. Though those eating very few carbohydrates do often see an increase in “bad” LDL cholesterol, it changes to the larger, fluffier kind of LDL that is not associated with cardiovascular disease.
For those of you that still follow the “low-fat” mantra – there is an overwhelming change in blood lipids in those eating fewer carbohydrates and more fat, which is associated with reduced risk of heart attacks and strokes. This isn’t seen in low fat dieters, despite their weight loss.
In order for our fat cells to lay down more storage material as extra “cushioning”, they need insulin. Insulin is the hormone that our bodies produce primarily in response to carbohydrates. Insulin turns off the mechanism by which the body burns its fat stores for energy (lipolysis). Insulin also switches on the enzyme lipoprotein lipase, which sucks up all the fat from the meal you just ate, and uses it to make some extra padding for your jeans.
It follows, then, that by not eating as many carbohydrates with our meals, we don’t get the associated increase in insulin, and fat cells don’t get their “storage” switch turned on. In fact, if you give people a large fatty meal, those that have been following a low carbohydrate/high fat diet will have lower levels of fat in the blood afterwards, because the body has become used to using fat directly as a fuel source.
While we’re here, don’t think you can cheat the system by drinking “diet” soft drinks. Artificial sweeteners can also cause an increase in insulin, despite not containing any “calories” or carbohydrate.
Protein, metabolism and calorie restriction
You can’t trick the body into sudden weight loss. Our bodies will use energy and burn fat based on our metabolism. This is affected by the amount and types of food we eat, the exercise we do, and the amount of energy it takes to keep our organs and muscles running. If you rapidly reduce the amount of food you eat, the body will automatically reduce its metabolism in order to prevent huge changes in weight. This often involves sacrificing our muscle tissue. Muscles provide a large portion of our metabolism, and a healthy metabolism is essential to achieve fat loss.
Chronic dieters who restrict calories tend to lose weight, which will include some muscle tissue. They will then re-gain the weight due to a combination of a slower metabolism, and the fact that forcing yourself to eat less is miserable. Over time, their percentage bodyfat increases, as cycles of weight loss result in less muscle and a slower metabolism.
This effect can be reduced by increasing protein in the diet. The combination of increasing protein and reducing carbohydrate during weight loss leads to an increased proportion of weight lost from fat rather than muscle. Those following low-carbohydrate, high-fat diets also have a better preservation of muscle mass and smaller reduction in metabolic rate compared to high-carbohydrate, low-fat dieters.
Protein has the bonus of making you feel full for longer by increasing a hormone called peptide YY, which improves feelings of satiety. Protein also does not induce the same insulin spikes and troughs which give you that feeling of being starving an hour after eating your breakfast cereal.
Diet as a noun rather than a verb
It is becoming more and more obvious that we must change the way we approach the whole idea of weight loss (or rather, fat loss). Focusing on calories doesn’t work, so trying to battle with them is a waste of time, and extra stress that you certainly don’t need. However, if we focus on eating for health, weight loss and longevity will happen automatically.
If we consider diet as the “habitual nourishment” that the dictionary says it should be, how should we eat? By no means do I suggest that everybody should live on an Atkins-style diet of only eggs and bacon. When we completely take out carbohydrates and only have fat to burn, the body produces “ketones”, which can also be used as fuel. Occasional mild “ketosis” appears to be beneficial in improving all our metabolic problems, but in extreme carbohydrate restriction, high ketone levels can actually stop the body burning its fat stores. For example, ketosis often happens in starvation, so the body’s natural response is to try and keep some fat for later, just in case.
The long-term sustainability of the way we eat is also incredibly important. Long-term “restriction” of anything makes adhering to a certain way of eating much harder. We therefore have to think about eating for the best improvement in health rather than trying to starve ourselves “healthy”.
Just reducing carbohydrates to provide less than a third of our energy improves weight loss, cholesterol and blood pressure.
The key is then to focus away from carbohydrate-heavy foods. These tend to be those that are the most highly processed which, ironically, increases the “calories” that you get from them. You could make a dramatic improvement simply by not eating bread, sweets/biscuits/cakes, breakfast cereal, or the traditional “meal bulkers” such as pasta, cous cous, rice or potatoes.
Pretty much everything else is still on the cards. A higher fat intake from fatty meat and fish, eggs, and some dairy (for those who aren’t intolerant), will help the body increase the use of fat as a source of fuel. The protein that comes with those foods will increase metabolism and feelings of satiety, which will mean you automatically eat less food over time. If you couple these with a good amount of vegetables, and some fruit and nuts, you will eat yourself to better blood pressure, weight loss, and lower your risk of cardiovascular disease, diabetes and obesity.
This can all be done without trying to starve ourselves by obsessing over calories. So go and grab yourself a nice big steak! You deserve it. Just don’t forget the side-salad.
References:
1. Hargrove JL. History of the calorie in nutrition. J Nutr. 2006 Dec;136(12):2957-61.
2. Novotny JA, Gebauer SK, Baer DJ. Discrepancy between the Atwater factor predicted and empirically measured energy values of almonds in human diets. Am J Clin Nutr. 2012 Aug;96(2):296-301.
3. American Association for the Advancement of Science (Monday, February 18, 2013: 9:45 AM-12:45 PM) http://aaas.confex.com/aaas/2013/webprogram/Session5859.html
4. Franz MJ, VanWormer JJ, Crain AL, Boucher JL, Histon T, Caplan W, Bowman JD, Pronk NP. Weight-loss outcomes: a systematic review and meta-analysis of weight-loss clinical trials with a minimum 1-year follow-up. J Am Diet Assoc. 2007 Oct;107(10):1755-67.
5. Feinman RD, Fine EJ. Nonequilibrium thermodynamics and energy efficiency in weight loss diets. Theor Biol Med Model. 2007 Jul 30;4:27.
6. Gross LS, Li L, Ford ES, Liu S. Increased consumption of refined carbohydrates and the epidemic of type 2 diabetes in the United States: an ecologic assessment. Am J Clin Nutr. 2004 May;79(5):774-9.
7. Basu S, Yoffe P, Hills N, Lustig RH. The relationship of sugar to population-level diabetes prevalence: an econometric analysis of repeated cross-sectional data. Am J Clin Nutr. 2004 May;79(5):774-9.
8. Heilbronn LK, de Jonge L, Frisard MI, DeLany JP, Larson-Meyer DE, Rood J, Nguyen T, Martin CK, Volaufova J, Most MM, Greenway FL, Smith SR, Deutsch WA, Williamson DA, Ravussin E; Pennington CALERIE Team. Effect of 6-month calorie restriction on biomarkers of longevity, metabolic adaptation, and oxidative stress in overweight individuals: a randomized controlled trial. JAMA. 2006 Apr 5;295(13):1539-48.
9. Brehm BJ, Seeley RJ, Daniels SR, D'Alessio DA. A randomized trial comparing a very low carbohydrate diet and a calorie-restricted low fat diet on body weight and cardiovascular risk factors in healthy women. J Clin Endocrinol Metab. 2003 Apr;88(4):1617-23.
10. Volek JS, Phinney SD, Forsythe CE, Quann EE, Wood RJ, Puglisi MJ, Kraemer WJ, Bibus DM, Fernandez ML, Feinman RD. Carbohydrate restriction has a more favorable impact on the metabolic syndrome than a low fat diet. Lipids. 2009 Apr;44(4):297-309.
11. Volek J, Sharman M, Gómez A, Judelson D, Rubin M, Watson G, Sokmen B, Silvestre R, French D, Kraemer W. Comparison of energy-restricted very low-carbohydrate and low-fat diets on weight loss and body composition in overweight men and women. Nutr Metab (Lond). 2004 Nov 8;1(1):13.
12. Ebbeling CB, Swain JF, Feldman HA, Wong WW, Hachey DL, Garcia-Lago E, Ludwig DS. Effects of dietary composition on energy expenditure during weight-loss maintenance. JAMA. 2012 Jun 27;307(24):2627-34.
13. Krieger JW, Sitren HS, Daniels MJ, Langkamp-Henken B. Effects of variation in protein and carbohydrate intake on body mass and composition during energy restriction: a meta-regression 1. Am J Clin Nutr. 2006 Feb;83(2):260-74.
14. Manninen AH. Very-low-carbohydrate diets and preservation of muscle mass. Nutr Metab (Lond). 2006 Jan 31;3:9.
15. Hite AH, Berkowitz VG, Berkowitz K. Low-carbohydrate diet review: shifting the paradigm. Nutr Clin Pract. 2011 Jun;26(3):300-8.
16. Anton SD, Martin CK, Han H, Coulon S, Cefalu WT, Geiselman P, Williamson DA. Effects of stevia, aspartame, and sucrose on food intake, satiety, and postprandial glucose and insulin levels. Appetite. 2010 Aug;55(1):37-43.
17. Batterham RL, Heffron H, Kapoor S, Chivers JE, Chandarana K, Herzog H, Le Roux CW, Thomas EL, Bell JD, Withers DJ. Critical role for peptide YY in protein-mediated satiation and body-weight regulation. Cell Metab. 2006 Sep;4(3):223-33.
It is becoming more and more obvious that we must change the way we approach the whole idea of weight loss (or rather, fat loss). Focusing on calories doesn’t work, so trying to battle with them is a waste of time, and extra stress that you certainly don’t need. However, if we focus on eating for health, weight loss and longevity will happen automatically.
If we consider diet as the “habitual nourishment” that the dictionary says it should be, how should we eat? By no means do I suggest that everybody should live on an Atkins-style diet of only eggs and bacon. When we completely take out carbohydrates and only have fat to burn, the body produces “ketones”, which can also be used as fuel. Occasional mild “ketosis” appears to be beneficial in improving all our metabolic problems, but in extreme carbohydrate restriction, high ketone levels can actually stop the body burning its fat stores. For example, ketosis often happens in starvation, so the body’s natural response is to try and keep some fat for later, just in case.
The long-term sustainability of the way we eat is also incredibly important. Long-term “restriction” of anything makes adhering to a certain way of eating much harder. We therefore have to think about eating for the best improvement in health rather than trying to starve ourselves “healthy”.
Just reducing carbohydrates to provide less than a third of our energy improves weight loss, cholesterol and blood pressure.
The key is then to focus away from carbohydrate-heavy foods. These tend to be those that are the most highly processed which, ironically, increases the “calories” that you get from them. You could make a dramatic improvement simply by not eating bread, sweets/biscuits/cakes, breakfast cereal, or the traditional “meal bulkers” such as pasta, cous cous, rice or potatoes.
Pretty much everything else is still on the cards. A higher fat intake from fatty meat and fish, eggs, and some dairy (for those who aren’t intolerant), will help the body increase the use of fat as a source of fuel. The protein that comes with those foods will increase metabolism and feelings of satiety, which will mean you automatically eat less food over time. If you couple these with a good amount of vegetables, and some fruit and nuts, you will eat yourself to better blood pressure, weight loss, and lower your risk of cardiovascular disease, diabetes and obesity.
This can all be done without trying to starve ourselves by obsessing over calories. So go and grab yourself a nice big steak! You deserve it. Just don’t forget the side-salad.
References:
1. Hargrove JL. History of the calorie in nutrition. J Nutr. 2006 Dec;136(12):2957-61.
2. Novotny JA, Gebauer SK, Baer DJ. Discrepancy between the Atwater factor predicted and empirically measured energy values of almonds in human diets. Am J Clin Nutr. 2012 Aug;96(2):296-301.
3. American Association for the Advancement of Science (Monday, February 18, 2013: 9:45 AM-12:45 PM) http://aaas.confex.com/aaas/2013/webprogram/Session5859.html
4. Franz MJ, VanWormer JJ, Crain AL, Boucher JL, Histon T, Caplan W, Bowman JD, Pronk NP. Weight-loss outcomes: a systematic review and meta-analysis of weight-loss clinical trials with a minimum 1-year follow-up. J Am Diet Assoc. 2007 Oct;107(10):1755-67.
5. Feinman RD, Fine EJ. Nonequilibrium thermodynamics and energy efficiency in weight loss diets. Theor Biol Med Model. 2007 Jul 30;4:27.
6. Gross LS, Li L, Ford ES, Liu S. Increased consumption of refined carbohydrates and the epidemic of type 2 diabetes in the United States: an ecologic assessment. Am J Clin Nutr. 2004 May;79(5):774-9.
7. Basu S, Yoffe P, Hills N, Lustig RH. The relationship of sugar to population-level diabetes prevalence: an econometric analysis of repeated cross-sectional data. Am J Clin Nutr. 2004 May;79(5):774-9.
8. Heilbronn LK, de Jonge L, Frisard MI, DeLany JP, Larson-Meyer DE, Rood J, Nguyen T, Martin CK, Volaufova J, Most MM, Greenway FL, Smith SR, Deutsch WA, Williamson DA, Ravussin E; Pennington CALERIE Team. Effect of 6-month calorie restriction on biomarkers of longevity, metabolic adaptation, and oxidative stress in overweight individuals: a randomized controlled trial. JAMA. 2006 Apr 5;295(13):1539-48.
9. Brehm BJ, Seeley RJ, Daniels SR, D'Alessio DA. A randomized trial comparing a very low carbohydrate diet and a calorie-restricted low fat diet on body weight and cardiovascular risk factors in healthy women. J Clin Endocrinol Metab. 2003 Apr;88(4):1617-23.
10. Volek JS, Phinney SD, Forsythe CE, Quann EE, Wood RJ, Puglisi MJ, Kraemer WJ, Bibus DM, Fernandez ML, Feinman RD. Carbohydrate restriction has a more favorable impact on the metabolic syndrome than a low fat diet. Lipids. 2009 Apr;44(4):297-309.
11. Volek J, Sharman M, Gómez A, Judelson D, Rubin M, Watson G, Sokmen B, Silvestre R, French D, Kraemer W. Comparison of energy-restricted very low-carbohydrate and low-fat diets on weight loss and body composition in overweight men and women. Nutr Metab (Lond). 2004 Nov 8;1(1):13.
12. Ebbeling CB, Swain JF, Feldman HA, Wong WW, Hachey DL, Garcia-Lago E, Ludwig DS. Effects of dietary composition on energy expenditure during weight-loss maintenance. JAMA. 2012 Jun 27;307(24):2627-34.
13. Krieger JW, Sitren HS, Daniels MJ, Langkamp-Henken B. Effects of variation in protein and carbohydrate intake on body mass and composition during energy restriction: a meta-regression 1. Am J Clin Nutr. 2006 Feb;83(2):260-74.
14. Manninen AH. Very-low-carbohydrate diets and preservation of muscle mass. Nutr Metab (Lond). 2006 Jan 31;3:9.
15. Hite AH, Berkowitz VG, Berkowitz K. Low-carbohydrate diet review: shifting the paradigm. Nutr Clin Pract. 2011 Jun;26(3):300-8.
16. Anton SD, Martin CK, Han H, Coulon S, Cefalu WT, Geiselman P, Williamson DA. Effects of stevia, aspartame, and sucrose on food intake, satiety, and postprandial glucose and insulin levels. Appetite. 2010 Aug;55(1):37-43.
17. Batterham RL, Heffron H, Kapoor S, Chivers JE, Chandarana K, Herzog H, Le Roux CW, Thomas EL, Bell JD, Withers DJ. Critical role for peptide YY in protein-mediated satiation and body-weight regulation. Cell Metab. 2006 Sep;4(3):223-33.
 RSS Feed
RSS Feed
{kind=link}